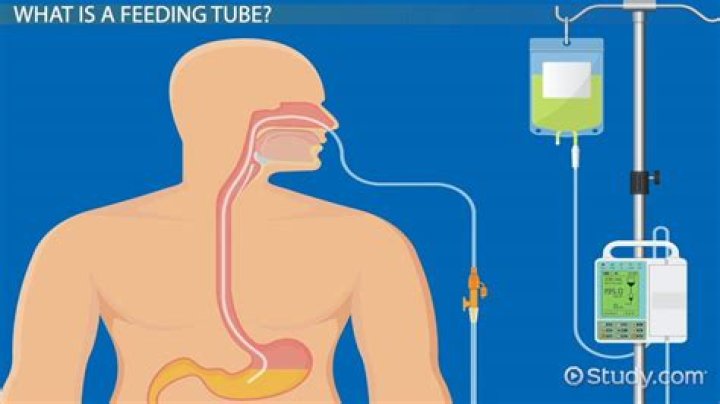
.
Also to know is, what does high residual mean in tube feeding?
Residual refers to the amount of fluid/contents that are in the stomach. Excess residual volume may indicate an obstruction or some other problem that must be corrected before tube feeding can be continued.
Secondly, why is tube feeding residual check? Therefore, expert bodies recommend we regularly "check residuals" on these patients, aspirating their stomach contents to see how much tube feeding is pooling there, and stopping the feeding if the volume seems high.
Also Know, how much residual is OK for tube feeding?
If using a PEG tube, measure residual every 4 hours (if residual is more than 200 ml or other specifically ordered amount, hold for one hour and recheck; if it still remains high notify doctor). If using a PEG tube, reinstall residual. Hang tube feeding (no more than 8 hours worth if in bag set up).
How do you prevent aspiration in tube feeding?
To minimize the risk of aspiration, patients should be fed sitting up or at a 30- to 45-degree semirecumbent body position. They should remain in the position at least one hour after feeding is completed. Iso-osmotic feeds may be preferred since high-osmolality feeds can delay gastric emptying.
Related Question AnswersWhat is a normal gastric residual volume?
Typically, standard nursing practice is to stop tube feedings due to gastric residual volume (GRV) that is twice the flow rate. So, a feeding rate of only 40 mL per hour would be held with a measured GRV of 80 mL. Normal gastric emptying occurs within 3 hours, slower for high fat meals and quicker for liquids.How often do you check tube feeding residuals?
If you are on continuous tube feeding, it is recommended that you check the residual at least every 8 hours. If you are on bolus feedings, it is recommended that you check residual before each feeding.What do you do with gastric residual?
For example, if a patient with a gastrostomy tube has a gastric residual volume of 100 ml or more, you may need to withhold feedings. Elevate the head of the bed to 30 degrees or greater for at least 1 hour after an intermittent feeding. Keep it elevated at all times for continuous feedings.What does a residual mean?
A residual is the vertical distance between a data point and the regression line. Each data point has one residual. They are positive if they are above the regression line and negative if they are below the regression line. If the regression line actually passes through the point, the residual at that point is zero.How do you find the residual for continuous tube feeding?
Check residual :- Wash your hands.
- Attach a 60cc catheter tip syringe to the feeding tube.
- Draw back on the plunger of the syringe to withdraw stomach contents or residual.
- However, if you pull back more than 150cc of stomach content, allow it to flow back in the stomach by gravity.
- Hold the feeding for 2 hours.
How do you aspirate gastric contents?
Attach a syringe to the nasogastric tube. Gently insert the nasogastric tube through the nose and advance it into the stomach. Withdraw (aspirate) gastric contents (2–5 ml) using the syringe attached to the nasogastric tube.How often do you flush a PEG tube?
Always flush your PEG tube before and after each use. Use at least 2 tablespoons (30 milliliters) of water to flush the tube. Follow directions for flushing your PEG tube.How do you give a bolus tube feeding?
In the meantime, you can:- Remove the plunger from the syringe.
- Put the tip into your feeding tube.
- Hold the syringe upright and fill it with 30 to 60 mL of water.
- Unclamp your feeding tube.
- Let the water drip in.
- When you no longer feel full, refill the syringe with the formula when the level gets low (see Figure 11).
What color is gastric residual?
Gastric aspirates were most frequently cloudy and green, tan or off-white, or bloody or brown. Intestinal fluids were primarily clear and yellow to bile-colored. In the absence of blood, pleural fluid was usually pale yellow and serous, and tracheobronchial secretions were usually tan or off-white mucus.Can you aspirate with a feeding tube?
As many as 40% of patients receiving enteral tube feedings aspirate the feedings into their lower respiratory tract, resulting in pneumonia. Dislodged or misplaced enteral feeding tubes, high gastric residual volume (GRV), dysphagia, and poor oral hygiene are all possible causes of aspiration pneumonia.How long should a bolus feeding take?
It may also be called syringe or gravity feeding because holding up the syringe allows formula to flow down using gravity. Most people take a bolus or a “meal” of formula about every three hours or so. This allows you to have more freedom in between feedings. A feeding will usually take up to 20 minutes.How do you know if a patient is tolerating a feeding tube?
Feed intolerance may present as vomiting, diarrhea, constipation, hives or rashes, retching, frequent burping, gas bloating, or abdominal pain. In very young children, prolonged crying and difficulty sleeping may be the only symptoms.How often must closed system tube feeding sets be changed?
This study suggests it is appropriate to change alimentation tube and feeding bags every 72 h (rather than every 24 h). The less frequent changes will decrease supply costs and free nursing time for other activities.What is the difference between enteral and parenteral?
Enteral nutrition generally refers to any method of feeding that uses the gastrointestinal (GI) tract to deliver part or all of a person's caloric requirements. Parenteral nutrition refers to the delivery of calories and nutrients into a vein.How do you calculate tube feeding?
On average, enteral formulas deliver between 1.0-2.0 calories/mL of formula. To calculate how much formula is needed, divide the total calorie needs by the amount of calories per mL of formula.How quickly can a stoma close?
The site will slowly close on its own over a period of about two weeks. Usually all that is needed is a bit of gauze to catch any initial leakage. Barrier cream can be used around the site to protect the skin from any leakage. Sometimes, the stoma or site does not close easily on its own.How do you gain weight with a PEG tube?
In an oral diet, you would first simply try eating more. The same idea applies to the enteral diet. If you use the bolus method for tube feeding, the most basic strategy to increase calories is to increase the volume of each bolus meal. Try slowly increasing a meal volume by 30- to 60-mL (1- to 2-ounce) increments.What is NG output?
Nasogastric intubation is a medical process involving the insertion of a plastic tube (nasogastric tube or NG tube) through the nose, past the throat, and down into the stomach. Orogastric intubation is a similar process involving the insertion of a plastic tube (orogastric tube) through the mouth.What are the most common complications of enteral feedings and how are these complications managed?
Pulmonary aspiration is an extremely serious complication of enteral feeding and can be life-threatening in malnourished patients.Aspiration
- Decreased level of consciousness.
- Diminished gag reflex.
- Neurologic injury.
- Incompetent LES.
- GI reflux.
- Supine position.
- Use of large-bore feeding tubes.
- Large gastric residuals.